

The DPC Starter Guide
1. Understand the DPC model before you build anything
Direct Primary Care is a membership-based primary care model. Patients, families, or employers pay the practice a recurring fee, usually monthly, in exchange for access to most routine primary care services. The practice generally does not bill insurance for the primary care services included in the membership.
A simple explanation patients can understand is:
"You pay one clear monthly fee for direct access to your primary care doctor, longer visits, simple communication, and transparent pricing. Insurance is still important for emergencies, hospital care, specialists, and services outside the membership."
Before choosing a name, logo, office, or software, define the promise of your practice. Your promise should be short and specific. For example:
Longer appointments without rushed visits.
Same-day or next-day access when medically appropriate.
Direct communication with the practice.
No insurance billing for included primary care services.
Transparent prices for membership and common outside services.
A smaller patient panel so the doctor has time to know patients well.
The strongest DPC practices are not just "cash-pay clinics." They are relationship-based primary care practices built around access, trust, and simplicity.

2. Choose your DPC structure
Decide what kind of DPC you are launching. The structure affects pricing, staffing, legal review, marketing, and the way you explain the practice.
Common models include:
Pure DPC: The practice charges a membership fee and does not bill insurance for covered primary care services.
Hybrid transition model: The practice keeps some insurance-based patients while gradually moving toward membership care.
Employer-focused DPC: Local businesses pay membership fees for employees as an employee benefit.
Micropractice DPC: A lean practice with one physician, minimal staff, low overhead, and a smaller panel.
Family-focused DPC: A model built around families, children, preventive care, and convenient access.
For most first-time founders, the simplest starting model is a lean, pure DPC practice with one physician, one support person or virtual assistant, clear pricing, and a defined panel cap. Hybrid models can work, but they often create confusion because the team has to manage two different businesses at the same time.
3. Validate the market before signing a lease
Do not assume people will join just because the model makes sense to you. Validate demand before taking on large fixed costs.
Create a list of at least 100 potential early supporters:
Current or former patients who value access and relationship-based care.
Self-employed professionals.
Families with high-deductible insurance plans.
Small business owners.
Local benefit brokers.
Gym owners, school leaders, church leaders, and community organizers.
Patients frustrated by long waits, rushed visits, or confusing bills.
Talk to them directly. Ask:
What frustrates you most about primary care today?
How long do you usually wait for appointments?
Do you understand your medical bills?
Would direct access and longer visits be worth a monthly membership fee?
Would your employer consider paying for this as a benefit?
What would make you hesitate to join?
Your goal is not to persuade everyone. Your goal is to identify the first 50 to 100 people who strongly understand the value. Those early members become your proof of demand.
4. Build the financial model first
DPC is a recurring revenue business wrapped around excellent medical care. The basic formula is simple:
Monthly revenue = active members x average monthly membership fee
Annual revenue = monthly revenue x 12
Estimated owner income = annual revenue - overhead
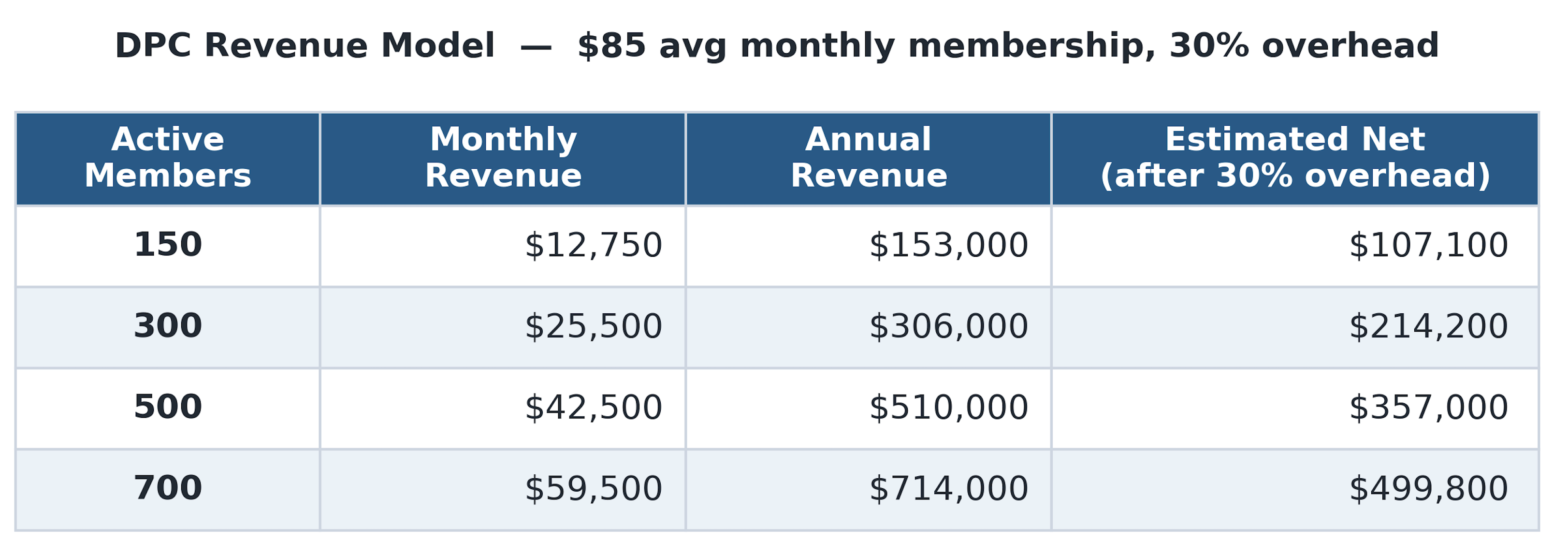
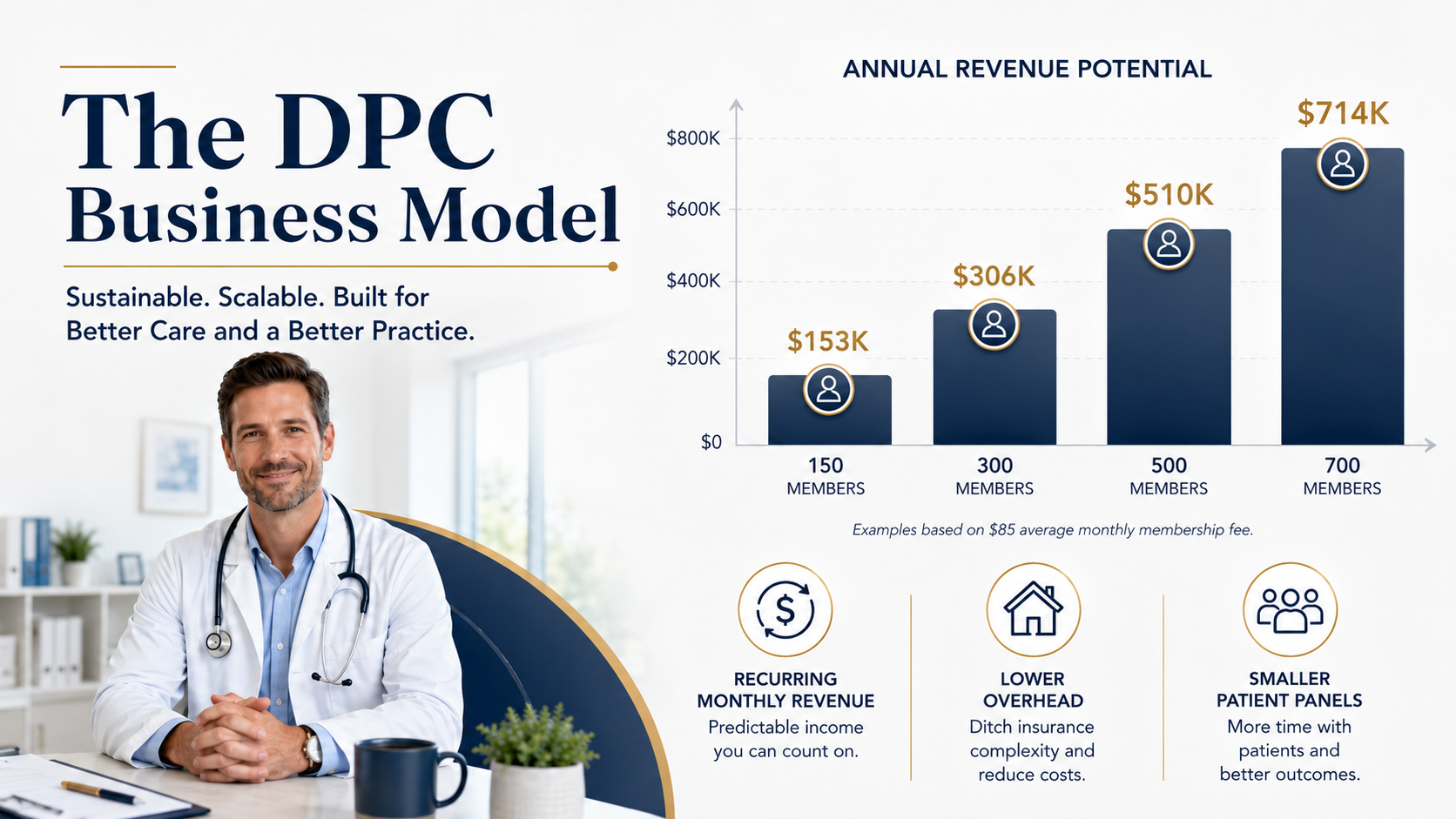
A realistic example using an $85 average monthly membership fee and 30% overhead:
Active MembersMonthly RevenueAnnual RevenueEstimated Net After 30%
The most important numbers are:
Average monthly membership fee.
Number of active members.
Monthly cancellations.
Overhead percentage.
Cash reserve.
Physician workload.
Do not price the practice so low that you need an oversized panel to survive. The point of DPC is not to recreate volume-based medicine with a different payment method. A strong early target is 300 members. A sustainable single-physician target may be 500 to 700 members depending on patient complexity, visit frequency, staffing, and access promises.
5. Create a pricing model patients can understand quickly
Your pricing should be simple enough to explain in ten seconds. Complicated pricing slows enrollment.
Example pricing structure:
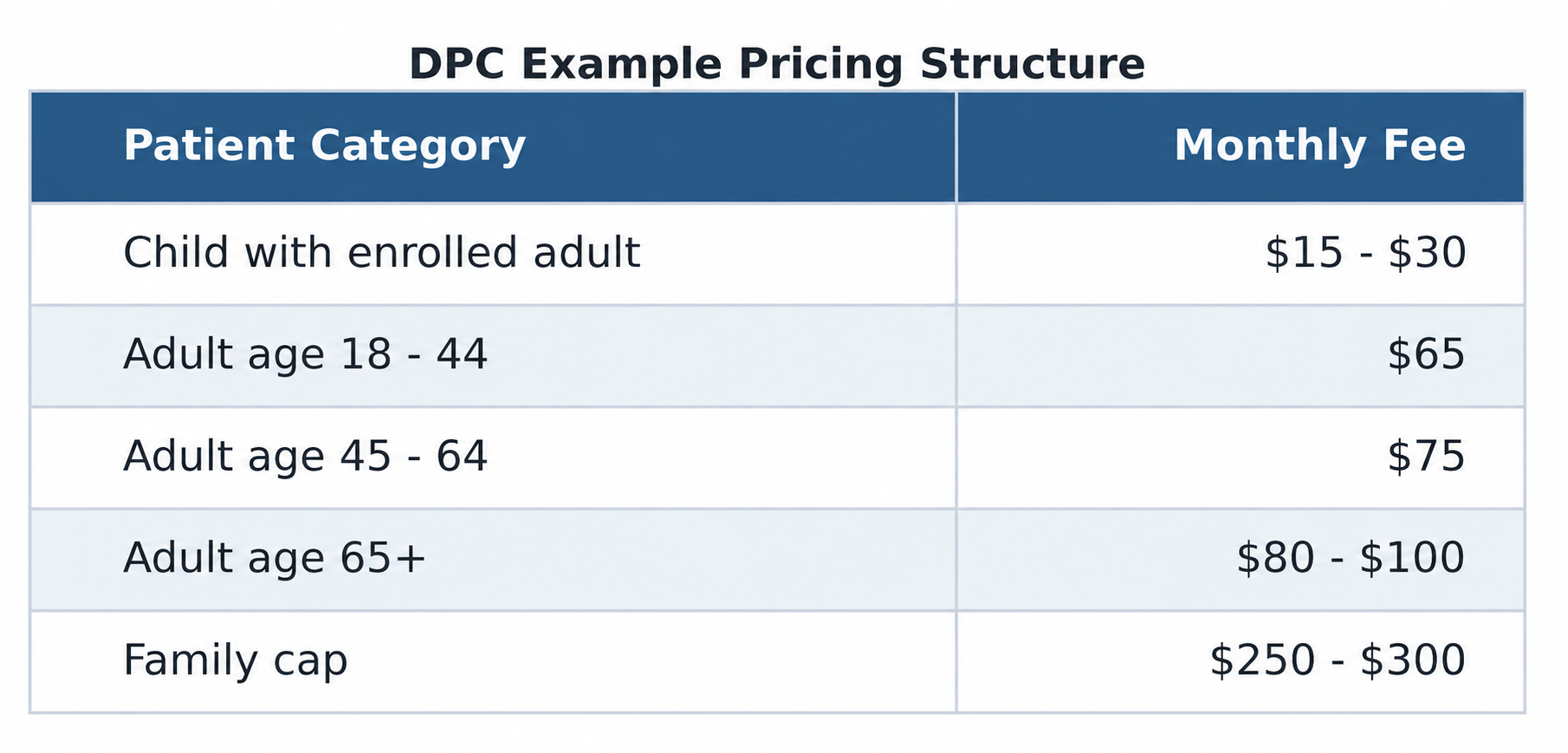
You may also charge a one-time registration fee, but keep it reasonable. Registration fees can help cover onboarding, records review, and initial administrative work, but a high fee can create unnecessary friction.
Pricing rules:
Publish pricing on the website.
Keep family pricing easy to understand.
Avoid too many exceptions.
Make cancellation terms clear.
Do not promise unlimited care in a way that creates unrealistic expectations.
Review HSA compatibility and state law before finalizing pricing language.
For employer groups, price per employee per month. You can offer tiers based on company size, but avoid creating custom complexity too early.
6. Define exactly what is included and excluded
Your membership agreement and website should clearly explain what the monthly fee covers.
Common included services:
Extended primary care visits.
Annual wellness and preventive visits.
Acute care visits for common illnesses and injuries.
Chronic disease management.
Medication management.
Direct messaging or phone access during defined hours.
Basic women's health services, if within scope.
Pediatric or adolescent care, if offered.
Simple in-office procedures.
Care coordination and specialist referral support.
Wholesale or pass-through lab coordination, if available.
Basic point-of-care testing, if properly licensed.
Common excluded services:
Emergency care.
Hospital care.
Specialist care.
Surgery requiring facility-level support.
Advanced imaging.
Outside laboratory, pathology, or imaging fees unless specifically included.
Medications, unless separately structured and legally reviewed.
Workers' compensation services, if not offered.
Disability evaluations, if not offered.
Controlled substance management, if limited by practice policy.
Patients should understand that DPC is not insurance. Many patients should still carry insurance for emergencies, hospitalization, specialists, major procedures, and services outside the DPC membership.
7. Handle legal setup before accepting patients
Before the first patient signs up, set up the business foundation correctly.
Core legal and business items:
Professional entity or other state-appropriate structure.
Employer Identification Number (EIN).
Business bank account.
Accounting system.
Malpractice coverage.
State medical license in good standing.
DEA registration, if prescribing controlled substances.
National Provider Identifier (NPI), even if not billing insurance.
Written DPC membership agreement.
Privacy policy and medical record policy.
Employment or contractor agreements.
Lease, sublease, or space-use agreement.
Lab, imaging, and vendor agreements.
Your DPC membership agreement should include:
A clear statement that DPC is not insurance.
Membership fee and billing cycle.
Services included and excluded.
Cancellation and refund terms.
Communication expectations.
After-hours and emergency care policy.
Patient responsibilities.
Physician termination rights.
Privacy and medical records language.
Employer-sponsored membership terms, if applicable.
Medicare/private contracting language, if relevant.
Do not copy another practice's contract and assume it works in your state. State DPC laws vary, and some states require specific patient protections or contract language.
8. Decide your Medicare position early
Medicare creates one of the biggest compliance decisions for a DPC founder. Decide your position before marketing to older adults or accepting Medicare beneficiaries.
Common options:
Do not accept Medicare beneficiaries at launch: This is operationally simple but limits your market.
Opt out of Medicare and use private contracts: This may allow private contracting with Medicare beneficiaries for covered services, but it must be done correctly.
Remain enrolled in Medicare: This may limit what you can charge Medicare patients privately for covered services.
If you opt out, Medicare rules generally require an opt-out affidavit and compliant private contracts with Medicare beneficiaries. A physician generally cannot opt out for some Medicare patients but not others, or for some covered services but not others. This area is technical. Get healthcare legal guidance before including Medicare beneficiaries in the DPC model.
9. Build compliance systems that match a medical practice
DPC reduces insurance billing bureaucracy, but it does not remove healthcare compliance obligations.
Set up these basics:
HIPAA-aware privacy and security policies.
Secure EHR and patient communication system.
Business associate agreements with vendors that handle protected health information.
Multifactor authentication.
Password manager.
Device encryption.
Role-based access for staff.
Secure backup process.
Breach response plan.
Medical record retention policy.
OSHA bloodborne pathogens exposure control plan, if staff have occupational exposure.
CLIA certificate, if performing applicable testing on human specimens.
Vaccine storage policies, if offering vaccines.
Biohazard waste and sharps disposal process.
Point-of-care testing is often useful in DPC, but do not begin testing without understanding CLIA requirements. Even waived tests may require a CLIA certificate. If employees may be exposed to blood or certain body fluids, OSHA's bloodborne pathogens rules may require a written exposure control plan.
10. Choose a lean technology stack
DPC practices need technology that supports membership care, not a bloated insurance billing workflow.
Core tools:
DPC-friendly EHR.
Recurring membership billing platform.
Online enrollment forms.
Online scheduling.
Secure messaging.
Business phone system.
E-fax or secure document exchange.
Website and landing page.
Email newsletter platform.
Accounting software.
Payroll software, if employing staff.
Secure cloud document storage.
Before choosing software, map the workflow:
Patient learns about the practice.
Patient reviews pricing.
Patient enrolls online.
Patient signs the membership agreement.
Payment method is collected.
New patient paperwork is completed.
Records are requested.
Initial visit is scheduled.
Follow-up plan is documented.
The fewer manual steps, the easier it is to grow without drowning in administration.
11. Set up the clinic space and operations
Start lean. A beautiful office is nice, but low overhead is more important in the early stage.
Minimum space needs:
One to two exam rooms.
Physician office or consult room.
Vitals station.
Phlebotomy or specimen collection area, if offered.
Vaccine refrigerator, if offering vaccines.
Secure medication or sample storage.
Clean waiting area.
ADA-compliant access.
Bathroom access.
Sharps and biohazard waste process.
Core supplies:
Exam tables.
Blood pressure cuffs and vitals equipment.
Otoscope and ophthalmoscope.
EKG, if offered.
Suture and procedure supplies.
Cryotherapy supplies, if offered.
Urine testing supplies, if offered.
Rapid test supplies, if offered.
Phlebotomy supplies.
PPE.
AED and emergency kit.
Staffing should stay simple. Many DPC practices can start with one physician and one medical assistant, part-time admin, or virtual assistant. Hire only when the bottleneck is obvious.
12. Build your cash-pay care network
One of the strongest benefits of DPC is helping patients access transparent pricing outside the membership.
Build relationships with:
Independent labs.
Imaging centers.
Local pharmacies.
Compounding pharmacies, when appropriate.
Specialists open to cash-pay pricing.
Physical therapists.
Mental health clinicians.
Dietitians and health coaches.
Employer benefit brokers.
Your goal is to create a practical local network. For example, when a patient needs labs or imaging, your team should know where to send them, what the approximate cash price is, and how results will return to the practice.
Be transparent about markups. Some DPC practices pass labs through at cost. Others charge a small administrative fee. Either can work if the policy is clear and legal in your state.
13. Design the patient experience
The patient experience is the product. Patients should feel the difference from the first interaction.
Create standards such as:
New patient visit: 45 to 90 minutes.
Routine visit: 30 to 60 minutes.
Same-day or next-day acute access when medically appropriate.
Clear response-time expectations for messages.
Annual care plan for each patient.
Follow-up reminders for chronic conditions.
Medication refill workflow.
Lab result communication workflow.
Referral tracking process.
After-hours boundaries.
Do not promise 24/7 unlimited access unless you truly have the staffing and lifestyle tolerance to support it. Clear boundaries protect the practice and the physician.
The best DPC practices feel calm, personal, and organized. Patients should not wonder how to reach you, what they owe, or what happens next.

14. Launch marketing 90 days before opening
Do not wait until the office opens to start marketing. Start building trust early.
90 days before opening:
Announce the practice.
Launch a simple website or landing page.
Publish the DPC explanation and pricing.
Start collecting email addresses.
Meet local business owners.
Contact benefit brokers.
Post educational content about how DPC works.
60 days before opening:
Open founding member enrollment.
Host small webinars or lunch-and-learns.
Share short patient-friendly FAQs.
Ask early supporters for referrals.
Begin employer conversations.
30 days before opening:
Schedule first visits.
Collect signed agreements and payment methods.
Send onboarding emails.
Request records.
Confirm workflows and supplies.
Test phones, messaging, scheduling, and billing.
Strong marketing messages:
"Longer visits. Direct access. Transparent monthly pricing."
"Primary care built around the doctor-patient relationship."
"No insurance billing for included primary care services."
"A better primary care experience for individuals, families, and employers."
Do not sell DPC as "cheap care." Sell it as better access, better relationships, and clearer pricing.
15. Add employer memberships
Employer groups can help a DPC practice grow faster, especially with small businesses that struggle with healthcare costs and access.
A simple employer pitch:
"We provide your employees with direct primary care access for a predictable monthly fee. The goal is faster care, fewer unnecessary urgent care visits, better chronic disease support, and a more attractive employee benefit."
Employer package options:
5 to 20 employees.
21 to 50 employees.
51 to 100 employees.
Custom pricing for larger groups.
Employer sales materials should include:
One-page explanation of DPC.
Pricing per employee per month.
What is included.
What is not included.
How employees enroll.
Privacy statement explaining that employers do not receive individual medical information.
Simple de-identified utilization reporting, if offered.
Protect patient privacy. Employers may receive aggregate, de-identified reports, but not individual medical details.
16. Track the numbers every month
A DPC practice should be relationship-driven, but it still needs disciplined business tracking.
Track monthly:
Active members.
New members.
Canceled members.
Net membership growth.
Average revenue per member.
Monthly recurring revenue.
Revenue by individual, family, and employer groups.
Visit volume.
Message volume.
No-show rate.
Panel complexity.
Overhead percentage.
Cash reserve.
Patient satisfaction.
Physician workload and burnout risk.
The most important question is:
"Is the practice becoming more sustainable while preserving the doctor's quality of life and the patient experience?"
If revenue is growing but the physician is becoming overloaded, adjust panel size, pricing, staffing, visit boundaries, or workflows.
17. Use this launch checklist
Before opening, confirm the following:
Business entity formed.
Business bank account opened.
Accounting system active.
Malpractice coverage active.
DPC agreement reviewed by healthcare attorney.
Medicare position decided.
HIPAA/security policies drafted.
EHR selected and tested.
Billing system tested.
Website live.
Pricing published.
CLIA certificate obtained, if testing.
OSHA exposure control plan created, if applicable.
Lab and imaging relationships established.
Phone and messaging systems live.
New patient forms complete.
Employer one-page pitch ready.
First 100 prospects contacted.
Founding member campaign launched.
First month of appointments scheduled.
18. First-year operating rhythm
The first year should focus on steady growth and operational discipline.
Monthly:
Review membership growth and cancellations.
Review cash flow and overhead.
Audit response times and patient access.
Ask for referrals from happy members.
Publish educational content.
Meet at least five potential referral partners or employers.
Quarterly:
Review pricing.
Review workload and panel capacity.
Review vendor performance.
Update patient FAQs.
Evaluate whether staffing needs have changed.
Review compliance tasks.
Annually:
Review membership agreement.
Renew malpractice and business policies.
Review privacy and security policies.
Update pricing if needed.
Revisit panel cap and growth strategy.
Survey patients.
Do not rush to scale before the model is stable. A calm, profitable 300-member practice is better than a chaotic 700-member practice that burns out the doctor.
Final advice
A successful DPC practice is simple, but it is not casual. The model works because the incentives are cleaner: patients pay directly for access to primary care, and the physician has more time to deliver thoughtful, relationship-based medicine.
The practices that win are disciplined about five things:
Clear pricing.
Low overhead.
Strong legal and compliance foundation.
Excellent patient experience.
Consistent local marketing.
You don't have to build all of this alone. CoreMed exists to make the hard parts of launching a direct primary care practice easier and to make the result better for the patients you'll serve. For most founders, the biggest early risk is an empty schedule. CoreMed helps fill it by connecting your new practice with members in your community who are already looking for exactly this kind of care, so you can open your doors with patients instead of starting from zero. You stay independent and run your own practice — we're simply the neighbor down the road helping you grow.
For patients, CoreMed turns a great idea into something easy to say yes to: one affordable monthly membership and a real relationship with a local doctor who has time for them. That simplicity is what makes membership medicine spread — people understand it, trust it, and tell their friends. If you've even thought about making the leap to your own DPC practice, reach out at [email protected]. We'd love to help you build it, and we have members ready to sign up.

Source and reference notes
Use these sources as starting points for legal, compliance, and operating review. Confirm current rules with counsel before launch.
American Academy of Family Physicians (AAFP): Direct Primary Care practice model, typical membership fees, DPC physician benefits, and DPC data brief.
Internal Revenue Service: Notice 2026-5 and related guidance on DPC service arrangements and HSA compatibility beginning January 1, 2026.
Centers for Medicare & Medicaid Services (CMS): Medicare opt-out and private contracting guidance.
U.S. Department of Health and Human Services (HHS): HIPAA Privacy and Security Rule guidance.
CMS CLIA program: Certificate requirements for testing on human specimens, including waived testing.
Occupational Safety and Health Administration (OSHA): Bloodborne Pathogens Standard, 29 CFR 1910.1030, and exposure control plan requirements.
